A Case Report Form is a structured instrument used to collect study data. It may be a paper form, an electronic form in REDCap, or a hybrid of both. The purpose of a CRF is not to reproduce the full medical record. Its purpose is to capture protocol-required data in a clear, consistent, and analysis-ready manner. Good CRF design reduces errors, supports efficient data entry, improves user experience, and strengthens the credibility of the final dataset.
The first principle is clarity. Questions should be written so that trained users interpret them consistently. A vague question such as “Patient status?” is poor because it does not specify whether the form is asking about hospitalization, survival, clinical condition, study status, or follow-up status. A clearer question would be “Participant hospitalization status at day.” The label should specify the concept, timepoint, and context where needed.
The second principle is necessity. Every field should have a reason to exist. A field may be necessary because it answers an objective, measures an outcome, determines eligibility, supports safety monitoring, documents protocol compliance, enables analysis, or supports governance. If no such reason exists, the field should be reconsidered. Unnecessary data collection wastes staff time and often increases missingness.
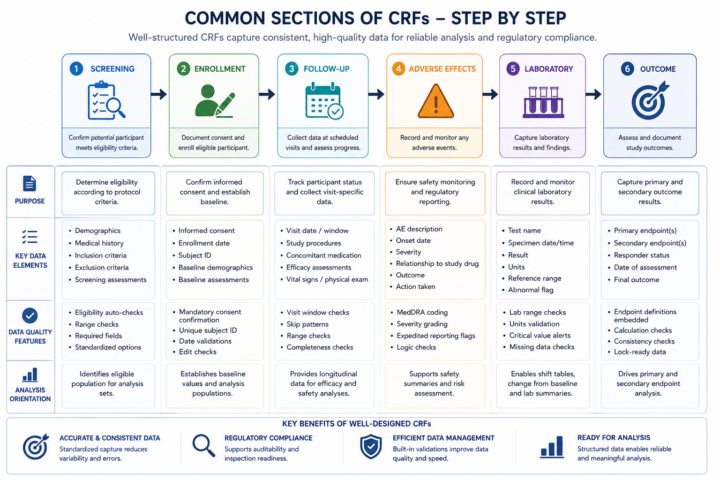
The third principle is logical flow. CRFs should follow the clinical or operational sequence in which data are collected. Screening forms should begin with consent and eligibility before enrollment decisions. Follow-up forms should place visit date and participant status before symptom or laboratory details. Adverse event forms should capture event description, onset date, severity, seriousness, relatedness, action taken, and outcome in a coherent order. Logical flow reduces user confusion and improves completeness.
The fourth principle is consistency. Similar concepts should be collected in similar ways across forms. Dates should use the same format. Yes/No variables should use the same coding scheme. Units should be consistently displayed. If one form records sex as “Male/Female” and another uses “M/F/Unknown,” the database becomes harder to clean and analyze. Consistency is especially important in large studies with many forms or sites.
The fifth principle is analysis readiness. Data should be captured in a format that supports planned analysis. Free text should be avoided for variables that need to be summarized or modeled statistically. Where possible, categorical variables should use coded options. Numeric variables should specify units and ranges. Dates should be captured as dates rather than text.
This does not mean that free text is never appropriate. Narrative fields may be necessary for adverse event descriptions or notes, but they should not replace structured fields required for analysis.
The sixth principle is user-centered design. Forms are completed by real people working under real conditions. If a form is too long, poorly ordered, or filled with unclear language, users may skip fields, enter placeholders, or make errors. Good design considers clinic workflow, time pressure, staff training, language, device size, internet connectivity, and source document availability. In electronic systems, branching logic can reduce burden by showing fields only when relevant.